The addendum was crafted partly in response to the concerns raised from hundreds of international GCP regulatory inspections. Some of the common clinical research site findings included:
- Inadequate records and / or record keeping
- Deviations from clinical trial protocols
- Improper storage, maintenance and / or archiving of records and essential documents
- Inadequate or non-existent quality management systems or standard operating procedures (SOPs)
- Inadequate, or poorly documented, training, education and qualification of clinical research personnel
- Inadequate or improper delegation of authority
- Inadequate access to source documentation
- Inadequate or non-compliant informed consent process or documentationGCP E6 R2 Addendum for Investigators Infographic
The amendment was introduced to encourage implementation of improved and more efficient approaches to clinical  trial design, conduct, oversight recording and reporting while continuing to ensure human subject protection and reliability of clinical trial results.
trial design, conduct, oversight recording and reporting while continuing to ensure human subject protection and reliability of clinical trial results.
The addendum introduces 26 new items, some related to sponsors, some to sites and some to both. In this article we will introduce the changes that will impact investigators and clinical research sites.
Click the Image to the right to view this content in infographic summary format
Certified Copies
NEW ITEM 1.63 “Certified Copy: A copy (irrespective of the type of media used) of the original record that has been verified (i.e., by a dated signature or by generation through a validated process) to have the same information, including data that describe the context, content and structure, as the original”
The first item we see in the addendum is the addition of the term “certified copy” into the ICH GCP glossary.
Site’s have been using certified copies for some time though we now see ICH standardizing the process. Certified copies are commonly used when providing medical records to monitors or inspectors, notably when they are not granted electronic medical record access.
A simple method often utilized at sites is to include a cover sheet to certify copies. We have included a job aide template with this article. Feel free to download, modify and use at your site!
Click Here to Download Certified Copy of Medical Record Cover Sheet Template
Media Types
The second and very prominent addendum to GCP impacting clinical research sites is in reference to media types. During the adoption and implementation of the last revision, GCP E6, most clinical trials were being conducted on paper. From medical records through to case report forms and beyond.
The addendum has added language throughout to specify that the guidance applies to all media types. Most prominently we see this with the addendum to one of the 13 principles of GCP.
NEW ITEM 2.10 “All clinical trial information should be recorded, handled, and stored in a way that allows it’s accurate reporting, interpretation and verification [ADDED “ This principle applies to all records referenced in this guideline, irrespective of the type of media used”]
Clinical Research Quality
Quality management holds a prominent place in this GCP E6 addendum. Focus has been placed on the implementation of quality management systems and risk based quality management.
NEW ITEM 2.13 “Systems with procedures that assure the quality of every aspect of the trial should be implemented [ADDED- Aspects of the trial that are essential to ensure human subject protection and reliability of trial results should be the focus of such systems”
For site’s this will mean implementation of a system to ensure that aspects essential to human subject protection and reliability of trial results are of the highest quality. Many smaller sites do not have a set of standard operating procedures, or guidance documents. In the new addendum sponsors have been tasked with focusing on quality. This will have sponsors looking to ensure that site’s have at least a bare minimum of SOPs or guidance documents. If you do not have basic SOPs already, consider some of the following:
- Informed Consent
- Screening / Enrollment
- Safety and SAE Reporting
- Source Documentation
- Essential Document Maintenance
- Study Staff Delegation and Training
Of course this list in non exhaustive and each sponsor may be looking to see other, or more specific, SOPs.
Delegation of Authority and Training
ICH has added two new items to the guideline pertaining to delegation of authority and training. Inadequate delegation and training continue to be major findings in GCP and regulatory inspections.
NEW ITEM 4.2.5 “The investigator is responsible for supervising any individual or party to whom the investigator delegates trial-related duties and functions conducted at the trial site”
NEW ITEM 4.2.6 “If the investigator / institution retains the services of any individual or party to perform trial-related duties and functions, the investigator / institution should ensure this individual or party is qualified to perform those trial-related duties and functions and should implement procedures to ensure the integrity of the trial-related duties and functions performed and any data generated.”
Beyond simple delegation GCP now calls for investigators to “supervise any individual or party to whom the investigator delegates trial-related duties and functions conducted at the trial site.
This extends the investigator’s responsibility beyond ensuring training and delegation, to continually supervising and documenting their oversight. It is no secret in the clinical research world that after delegation many investigators will not revisit the assigned tasks and assume they will be completed accurately unless told otherwise, say by the monitor.
A great place to document the process for continued oversight would be in your Study Staff Delegation and Training SOP referenced above!
Site’s should ensure that all meetings and communications between the investigator and delegated study staff are documented. This should include telephone calls, texts, study meetings, eligibility discussions etc…
Source Documentation ALCOA
ALCOA has been a “household” term in clinical research for years. We now see that GCP has adopted ALCOA into their Good Clinical Practice guidance.
ALCOA Clinical Research Training
As we know ALCOA stands for:
Attributable: It should be clear who has made the entry
Legible: The entry must be 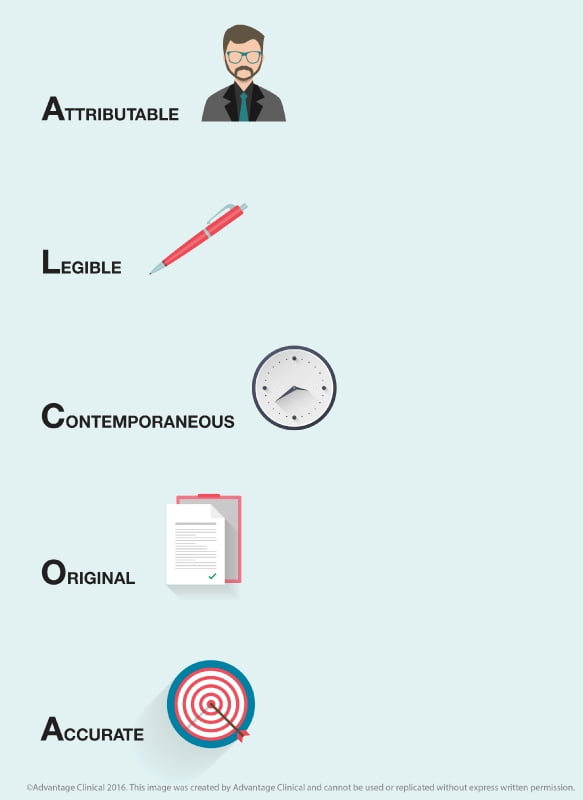
readable
Contemporaneous: The entry must indicate both when the event occurred as well as when it was entered.
Original: The entry must be the first place the information was recorded.
Accurate: The entry must reflect what occurred.
GCP has also clearly specified in the addendum the need to create an audit trail whereby changes to source data are traceable, should not obscure the original entry, and should be explained if necessary.
NEW ITEM 4.9.0 “The Investigator/institution should maintain adequate and accurate source documents and trial records that include all pertinent observations on each of the site’s trial subjects. Source data should be attributable, legible, contemporaneous, original, accurate and complete. Changes to source data should be traceable, should not obscure the original entry, and should be explained if necessary (e.g., via and audit trail).
Source and Essential Documentation Location
NEW ITEM 8.1 “The sponsor and investigator should maintain a record of the location(s) of their respective essential documents including source documents. The storage system used during the trial and for archiving (irrespective of the type of media used) should provide for document identification, version history, search and retrieval…”
The implications for this addition to the guidance will be far reaching for sites. Notably that sites must maintain a record of the location of source documents during the trial. For many sites their medical records may not be compiled in one location. For example medical images may be located in a separate department, CVs may be stored with HR or in a separate binder from the ISF, and so on.
A simple way to align your site with this guidance would be to compile a listing of the locations of all source and essential documents, and note their location in your Essential Documents SOP. Beyond study conduct this new item puts more structure around the archival of all source and essential documents pertaining to a particular trial.
Data Ownership
The last and final item pertaining to investigators and clinical research sites is in reference to data ownership. ICH has clearly stated that investigators should retain control and continuous access to the case report form data which has been reported to the sponsor.
NEW ITEM 8.1 “… The sponsor should ensure that the investigator has control of and continuous access to the CRF data reported to the sponsor. The sponsor should not have exclusive control of those data…”
We have incorporated all of these and the updated sponsor requirements into our Good Clinical Practice training course. This course is available online and has been recognized by Transcelerate to enable mutual recognition of Good Clinical Practice Training between sponsors, CROs and sites.
Click here to view our Good Clinical Practice Training in our course catalogue.
This revision to Good Clinical Practice has been a long time coming and we are seeing sponsors, sites and regulatory authorities already begining to take action to align themselves with the addendum. We hope you have found this article helpful in understanding the impacts of this revision at your research site!